The 7Cs+ Greater Triangle Learning & Action Network is a multi-county collaborative among community-based organizations (CBOs), public health and social agencies, healthcare providers, system leaders, and payers. The network consists of the following contiguous North Carolina counties aligned with NC DHHS Medicaid Region 4:
| Durham | Orange | Wake |
| Franklin | Person | Warren |
| Granville | Vance |
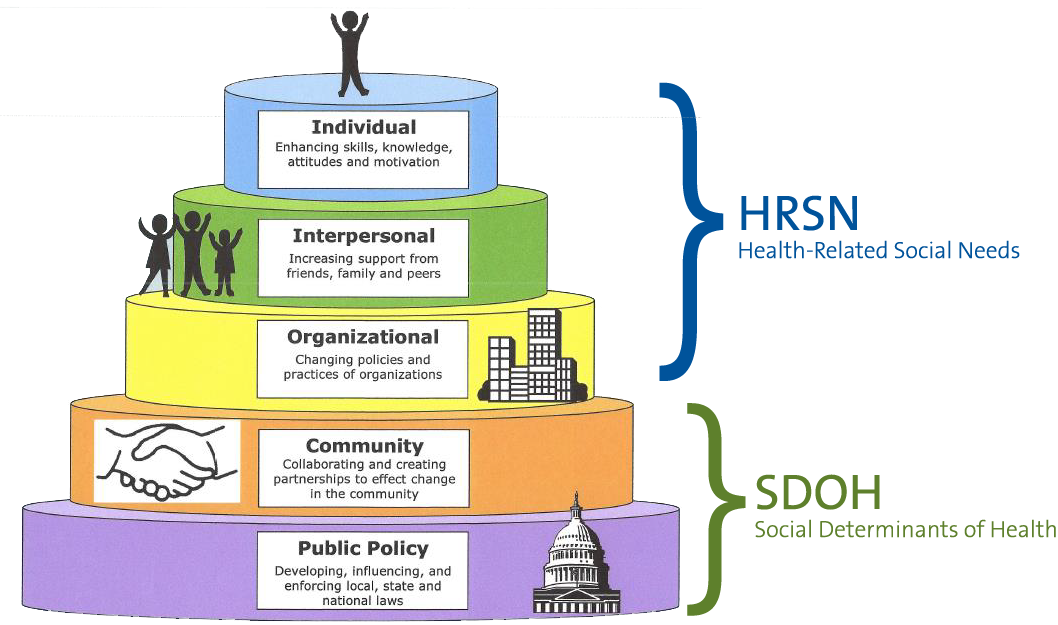
Social Determinants of Health (SDOH) and Health Related Social Needs (HRSN) in the context of the Socio-Ecological Model, explains that the different Greater Triangle stakeholders are primarily engaged in implementing specific HRSN interventions; whereas, Greater Triangle stakeholders collaborate with each other within the framework of “Community” and “Public Policy.” Click HERE to download the White House SDOH Play Book.
Mission
To act locally while incorporating or establishing regional policy-making constructs within each of the five major SDOH domains to improve equity in social care and health care:
- Food Security
- Housing
- Transportation
- Financial Assistance
- Interpersonal Violence
Vision
To be an effective regional voice and partner in developing solutions that meaningfully improve health outcomes in our region
Goal
Enhance integration of social care and health care with the belief that it will improve Health and Racial Equity.
“Giving families and Individuals what they need when they need it”
Guiding Principles
- Operate within an asset-based approach that focuses on prevention not just intervention and listening to community members to better understand their needs/challenges.
- Achieving Equity is foundational to improving health. We believe that financial, social, environmental, and racial inequities affect the health, well-being and upward mobility of families and communities.
- Historical and persistent poverty, segregation, disinvestment are manmade constructs reverberating daily throughout our community; reflected in human and property violence. We will advocate for local action that focus on high Social Vulnerability Index (SVI) census tracts.
- We will work across family, community, organizational and geographic boundaries as we advocate, design, and implement the integration of social care and health care. As we design solutions, we will account for and support the varied charitable eco-systems. We believe opportunities and solutions come from within the different eco-systems within and across urban, suburban and rural counties.
- We will move upstream to improve community conditions with laws, regulations and policies that support health for all people. (CMS is active in establishing SDOH and equity polices, and continues to promote “evidence-based” screening and resolution policies without specifying a specific standard/protocol).
- Promote harmonization and consistency with national/CMS policies, mindful of the national strategy and standards that we anticipate will be emerging.
- Global and discrete manifestations of structural racism are associated with residential neighborhood health. Discrete neighborhood constructs may represent promising targets for interventions seeking to mitigate the negative health effects of structural racism.
- Continually evaluate and improve our “First Big Steps”: including Systematic roll out of SDOH screening across health care providers; systematic rollout of resource and referral close loop platform across health care providers and CBO’s; understanding that United Way, NC DHHS and each health care system (UNC, Duke and Wake Med) have endorsed utilization of NCCARE360.
- Work together to increase capacity of CBOs to serve our historically disenfranchised populations.